

Doing any coronary intervention such as PTCA involves giving intra arterial iodinated contrast which is toxic to the kidneys, especially if the patient has already compromised renal function, is diabetic and or is on nephrotoxic drugs. Contrast induced nephrpopathy(CIN) is an iatrogenic complication which carries significant morbidity and mortality risk to the patient, independent of their underlying condition. Because of this issue, various predictive and therapeutic strategies have been made including risk prediction scores, various medications, but the only proven strategy with clinical evidence of benefit has been adequate hydration of the patient pre and post procedure ( which again is limited by LV function) and use of isoosmolar contrast mediums.
The dream of doing procedures with minimal or zero contrast to obviate the risk of CIN, is now possible with the availability of intracoronary imaging, and this may be the beat way to prevent this complication. One such case dine recently by us is described:
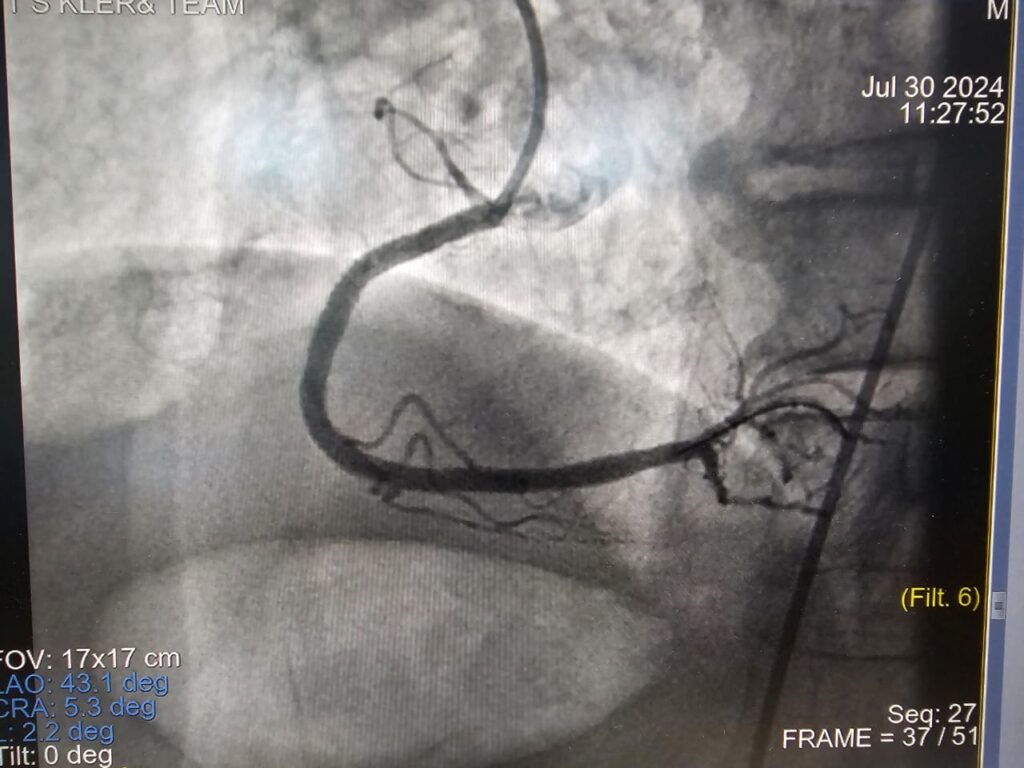
Mr DD, 85 M, was worked up at another hospital for Urology surgery and found to have strongly positive DSE and subsequently underwent angiography which revealed a critical lesion in proximal RCA followed by long segment of the vessel which had disease extending to the distal vessel. The issue was patient had a Creatinine of 4.1mg/dl, putting this patient at very high risk for developing CIN post angioplasty. After discussing and informed consent from the patient and attendants we planned a minimal/zero contrast PTCA procedure.
The entire procedure was done with intravascular ultrasound (IVUS) guidance. Blind intubation and wiring of the vessel was done, and IVUS guidance obtained for sizing, length and distal and proximal positioning of stents. Pre-dilatation and stent placement were also done successfully and final expansion checked with IVUS. A final short angiogram was done to confirm and patient wheeled out. Total contrast used was 10 ml, as oppposed to about 150 ml usually. Patient had pre procedure Creatinine of 3.81mg/dl and next morning it was 3.80.
This technique of minimal contrast PTCA is a very useful addition to our armamenterium in preventing CIN and involves expertise in interpretation of IVUS imaging to guide stent sizing, placement, and post stent assessment.
PTCA done with only 10 ml contrast to save further damage to kidneys of patient with compromised kidney function and raised Creatinine level.